Original post published on 8th January 2022 by Giuseppe Natalini
Last week I published a 7 second long strip showing pressure and flow curves from a mechanically ventilated patient, asking you to anonymously suggest an interpretation. This week about a thousand people have read the post, and fifty people have given their own interpretations on the traces.
I read with great attention all the answers, and I noticed one thing: almost all of ventilab’s readers have focused their attention on aspects which were different from the one I had planned to discuss. It’s amazing how many things only 7 seconds of pressure and flow curves monitoring can tell us! I am really happy to have let you express yourselves on the matter before I did. Listening before talking lets me offer different levels of interpretation for this short strip, making the discussion more exhaustive.
I have decided to publish a series of close up posts in which we will evaluate all the considerations that ventilab’s readers have written on the form from 29/12/2021’s post.
I will leave the post explaining why this monitoring has attracted my attention and how this permitted me to find and solve the problem for last.
Today we will see what these 7 seconds can tell us on the modality of ventilation and on the ventilator's settings.
What is the ventilation modality and what are the ventilator settings?
Recognizing the ventilation modality and ventilator settings from graphical monitoring (that is to say, from simple pressure and flow traces) means to have truly understood mechanical ventilation. It is an exercise that I suggest to ALWAYS do: it's the only way to reach an understanding of the real way mechanical ventilation works, overcoming the blanket of smoky clouds that often is an obstacle to correct interpretation.
Figure 1 shows the original image:
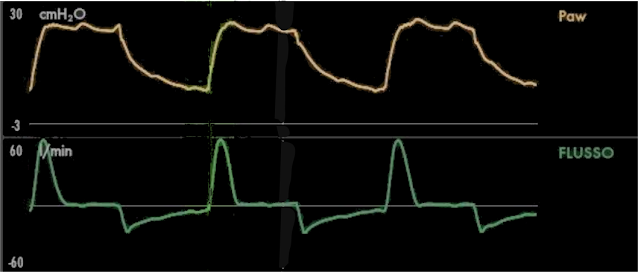
Figure 1
Ventilator settings have been estimated as an inspiratory pressure approximately between 25 and 28 cmH2O and a PEEP between 5 and 7 cmH2O: reasonable answers, since from the images it was not possible to be more accurate. In reality, applied pressure was 24 cmH2O and PEEP was 6 cmH2O.
It was noted that the duration of inspiration and expiration is similar, therefore I:E ratio is 1:1 and respiratory rate is around 25 breaths/minute. Calculation of respiratory rate is simple: in about 7 seconds we see almost 3 breaths (only the last part of the expiration is missing from the last breath). Dividing 7 seconds by 3 I obtain the duration of a single breath (2.33”) rounded down, I then round it up to 2.4”. If a breath lasts about 2.4”, respiratory rate is about 25 breaths/min, with an inspiratory time of 1.2” and an expiratory time lasting the same. Having said that tidal volume was 230 ml, minute ventilation was 5.75 l/min.
The proposed ventilation modalities were: pressometric ventilation, pressure-controlled ventilation, volume-targeted pressure-controlled ventilation, assisted-controlled pressometric ventilation, APRV.
All these answers might be right, but only one is certainly correct: the set ventilation is generically a pressometric ventilation, and there are no elements that permit answering more precisely. Pressometric ventilation is characterized by constant inspiratory pressure and decreasing inspiratory flow, and both of these features are present, as you can see in the “insp” portion of Figure 2:

These characteristics are common for all the pressometric ventilations. Since all ventilation modalities except volume-controlled, NAVA and PAV are pressometric, we haven’t taken such a big step forward.
Another consideration arises from this one: if almost all ventilation modalities are pressometric, does the modality of ventilation really matter? As those of you who have followed some of our courses well know, I believe that the modality has little importance, but its correct setting is of prime importance. In other words, a patient can be managed indifferently well with different ventilation modalities if for each one of them the ventilation parameters are set well. At the same time, a patient can be inadequately ventilated using each ventilation modality if its settings are not appropriate.
To say that a patient is ventilating with pressure support ventilation (or any other modality) is an information that has little value unless we specify how much support is applied, how much tidal volume and respiratory rate are generated, what does the flow profile look like, if any asynchronies are present and eventually which ones, how is the thoraco-abdominal coordination, if accessory inspiratory muscles are being used.
Going back to our clinical case, we can say that this ventilation is pressometric. In the family of pressometric ventilations, we can exclude one with certainty: pressure support ventilation. This is because during the inspiratory time we can see a pause, which can NEVER exist during pressure support ventilation because flow cycling makes sure that inspiration ALWAYS stops when there is still inspiratory flow (see 27/12/2017 post).
From the images we cannot tell if it is a pressure-controlled or a volume-targeted pressure-controlled ventilation (called PCV-VG, PRVC, IPPV with autoflow, APV, PC-target vent, volume adaptive BiLevel, et cetera in different ventilators): in case of a passive patient, the two ventilations are indistinguishable using graphical monitoring since they are both pressure-controlled ventilations. The difference can be seen only by looking at the settings panel: in pressure-controlled ventilation you set the applied pressure (and the tidal volume is variable), while in volume-targeted pressure-controlled ventilation you set desired tidal volume and the ventilator does a variable pressure-controlled ventilation, changing constantly the applied pressure in order to obtain the desired volume. In our example, it was a volume-targeted pressure-controlled ventilation, that is the desired tidal volume was 230 ml.
Assisted-controlled pressometric ventilation is a controlled pressometric ventilation in which the trigger is activated by the patient. Can you see trigger activation in Figure 1? If so, it is an assisted-controlled ventilation, if not it is a controlled ventilation. Patient-ventilator interaction will be discussed in the next post.
Finally APRV (Airway Pressure Release Ventilation) was suggested as a possible set ventilation modality (for more information see the 11/02/2015 post). APRV is a BIPAP, meaning that it alternates between two pressure levels that let the patient spontaneously breathe in any phase. In other words, it is the alternation of two CPAPs. Differently from BIPAP (which is defined as a partially asynchronous ventilation), APRV should be completely asynchronous, not taking into account the patient’s spontaneous breathing activity in the rythmic alternance between a higher pressure (Phigh) and a lower pressure (Plow). The rationale behind this approach is interesting (synchronicity is not always good), and we can discuss it in comments if you find it interesting.
Typically, APRV should be set with a significantly longer time at Phigh than at Plow. If the ventilation shown in Figure 1 was an APRV, Phigh (which would coincide with “insp” in Figure 2) would be 25-28 cmH2O and Plow (which would coincide with “esp” in Figure 2) would be 5-7 cmH2O, and both would last 1.2”: a possible choice, even if not typical for APRV. The ripples seen on the pressure curve at Phigh would have to be interpreted as signs of the patient's spontaneous respiratory activity. As we have said before, the set ventilation was a volume-targeted pressure-controlled ventilation, but from the shown image it was reasonable to think it was an APRV.
Here we end our exercise involving reading mechanical ventilation from flow and pressure curves. We will go on next week by discussing the many comments you made on patient-ventilator interaction.
As always, a smile for all of ventilab’s friends.
No comments:
Post a Comment