Original post written on 31st March 2021 by Giuseppe Natalini

An increase in dead space reduces alveolar ventilation in absence of an adequate increase in minute ventilation. When this happens, PaCO2 increases. Nonetheless, hypercapnia is not only caused by an increase in dead space, but it can also be secondary to a reduction in minute ventilation (see 17/02/2018 post).
Today’s post focuses on this complex relationship between dead space, hypoventilation and hypercapnia and offers two simple dead space surrogates (corrected minute ventilation and Ventilatory Ratio).
Minute ventilation, alveolar ventilation, dead space and PaCO2
We are used to measuring a patient’s ventilation as minute ventilation (VE), that is to say the product of tidal volume (VT) and respiratory rate (RR), which quantifies how many liters of air come in and out of the airways in 1 minute. A healthy subject, as it is taught by physiology, inhales 0.5 L of VT, about 12 times per minute. This means that his\her VE is 6 L/min.
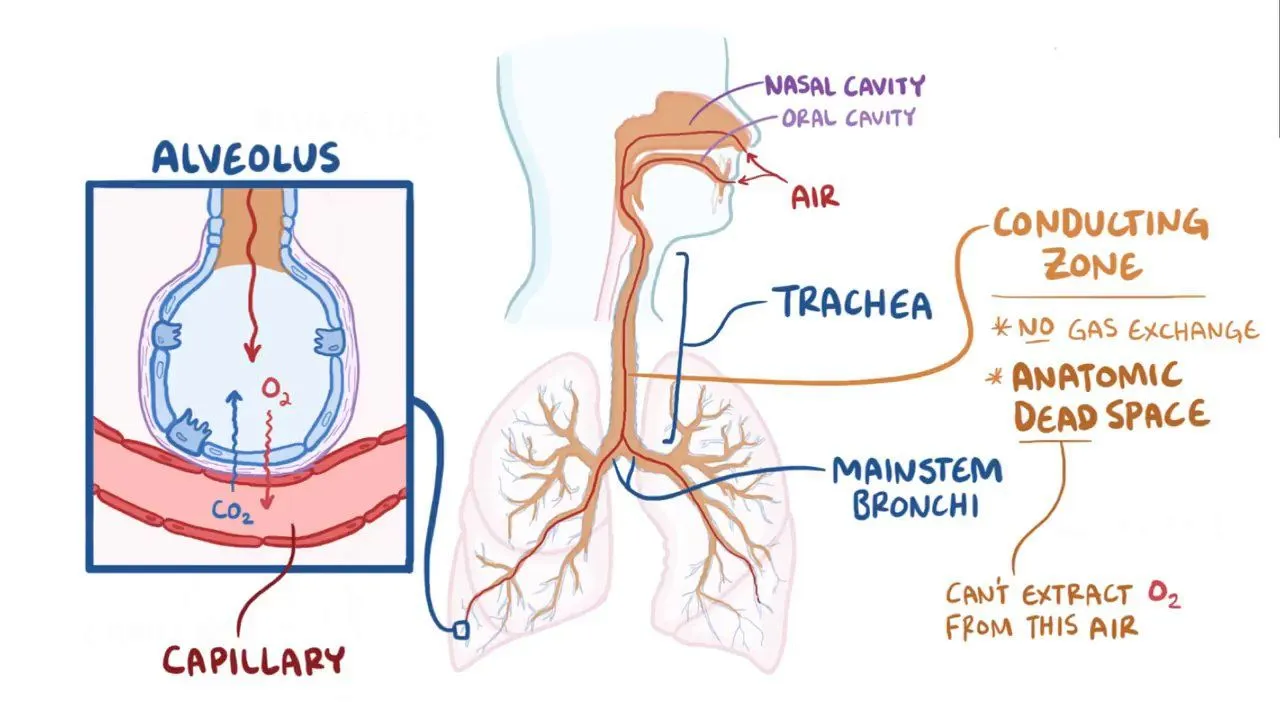
PaCO2 depends on the quote of VE that we call alveolar ventilation (VA). Dead space ventilation (VD) is the difference between VE and VA, that is to say the quote of VE that does not take part in gas exchange. In physiology, dead space is identified only by the volume of air that stays in the airways (anatomic dead space), which is about 150 mL.
VA is therefore calculated as:
VA = (VT - VD) ∙ RR
In a healthy male subject, which we are going to call -in an original way- Mario Rossi, we can calculate the VA using the above mentioned data:
VA = (0.5 L - 0.15 L) ∙ 12/min = 4,2 L/min.
PaCO2 is inversely proportional to VA:
PaCO2 ~ 1/VA
and Mario Rossi has a normal PaCO2 of 40 mmHg with a VA of 4,2 L/min, which corresponds to a VE of 6 L/min.
Hypoventilation.
The previous formulas tell us that, if Mario Rossi’s respiratory frequency is halved (from 12 to 6 breaths/min), VA becomes half of the previous one, and therefore PaCO2 doubles to 80 mmHg.
It’s an easily handled situation: to go back to a PaCO2 of 40 mmHg, it is enough to start mechanical ventilation, setting a respiratory rate of 12 breaths/min and a tidal volume of 500 mL, which is what all anesthesiologists do when they induce general anesthesia.
Hypoventilation is the least important problem for those who know how to handle mechanical ventilation, unless intubation fails or unless airway obstruction is present...
Dead space
Let’s say that Mario Rossi is affected by ARDS and that he is ventilated with a tidal volume of 430 ml and a respiratory rate of 28 breaths/min. With these settings, the VE is 12 L/min (two times the norm) and, if dead space had remained 150 ml, VA would be 7.8 L/min (almost two times the norm) and therefore PaCO2 would be almost half the norm (a little over 20 mmHg).
But we all know very well that reality is different from this: if Mario Rossi has ARDS, he can have hypercapnia despite the increase in VA and VE.
In ARDS, alveolar dead space (which is negligible in physiology) increases, representing the air volume that does not take part in gas exchange even if it is contained into the alveoli. Alveolar dead space is generated if there are alveolar surfaces that do not receive pulmonary capillary perfusion or if the lungs are characterized by an increase and heterogeneity in ventilation/perfusion ratio.
In ARDS, physiologic dead space, i.e the sum of alveolar and anatomic dead space, can reach 80% of tidal volume. With this dead space value, it is possible to calculate that Mario Rossi has a PaCO2 of 70 mmHg, despite hyperventilation.
Differently from the one caused by hypoventilation, hypercapnia due to an increase in dead space is particularly difficult to fix, because a great increase in VE, obtained by increasing tidal volume and respiratory rate, would be required. These are choices that can assist in generating Ventilator-Induced Lung Injury: a solution much worse than the (presumed) problem we want to solve.
In this case it is better to accept hypercapnia, which is more of a marker of severity than a problem, and wait for it to resolve after the patient gets better.
Dead Space Surrogates
Dead space is the variable most associated with mortality in ARDS patients. Its knowledge can have a prognostic value, it can help correctly understand hyperventilation and hypercapnia, and can be useful in the evaluation of the evolution of ARDS when both VE and PaCO2 vary. Dead space, in the evaluation of ARDS patients, should at least be placed side-by-side to the well known PaO2/FIO2, which as we know has many limitations (see 29/01/2017 post)
However, dead space calculation requires the measurement of mean CO2 partial pressure in expired gas, which is not often available since it requires appropriate instruments such as volumetric capnography or indirect calorimetry.
Nonetheless we have the possibility to use two surrogates of measured dead space: corrected VE (VEcorr) and Ventilatory Ratio. Although both of these indexes have the limit of using VE as an indicator of VA (we have seen it is not the same thing), they have been found to be associated with prognosis in ARDS patients, similarly to dead space. They can therefore be useful surrogates of dead space in clinical practice.
Corrected minute ventilation (VEcorr)
VEcorr shows how much VE should be in order to have normal PaCO2.
It is easy to calculate:
VEcorr = VE ∙ PaCO2/(physiological PaCO2),
where physiological PaCO2 is estimated as 40 mmHg.
If a subject has a normal PaCO2, VE e VEcorr are the same.
Now let’s calculate Mario Rossi’s VEcorr when he hypoventilates and when he has ARDS, as described in the two previous examples.
When Mario Rossi hypoventilates:
VEcorr = 3 L/min ∙ 80 mmHg/40 mmHg = 6 L/min
In this example VEcorr is the same as the VE "in physiology books”, and we can conclude that dead space is absent. Good news for the patient (a low dead space is associated with a lower probability of death) and an easily corrected condition.
In ARDS patients, VEcorr is associated with an increased mortality when it is higher than 13 L/min.
Let’s calculate VEcorr in Mario Rossi with ARDS:
VEcorr = 12 L/min ∙ 70 mmHg/40 mmHg = 21 L/min
This means that Mario Rossi should have a VE of 21 L/min in order to have a PaCO2 of 40 mmHg: a really high value, which indicates a severe increase in dead space. This is bad news for Mario Rossi and a condition that should induce us to tolerate hypercapnia as the lesser evil compared to an escalation in ventilation.
Ventilatory Ratio
Ventilatory Ratio indicates how many VE should be increased, compared to the ideal value, in order to reach normal PaCO2. Differently from VEcorr, Ventilatory Ratio is an adimensional number which considers also the level of ideal VE, which in turn depends on the patient's height. Ideal VE is thought to be 0.1 L/min per kg of ideal body weight.
A small person, with an ideal body weight of 48 Kg, has an ideal VE of 4.8 L/min, much different from the 8 L/min which represent the ideal VE ideale of a person 185 cm tall and with an ideal body weight of 80 kg.
Ventilatory Ratio is calculated as:
Ventilatory Ratio = VE/(ideal VE) ∙ PaCO2/(ideal PaCO2).
As we have said above, the ideal VEis calculated as 0.1 L/min per kg of ideal body weight, and ideal PaCO2 is estimated as 37.5 mmHg.
In the case of Mario Rossi, who has an ideal body weight of 70 kg, Ventilatory Ratio when he hypoventilates is calculated as:
Ventilatory Ratio = 3 L/min / 7 L/min ∙ 80 mmHg/ 37.5 mmHg = 0.9.
That means that Mario Rossi needs a VE equal to 0.9 the ideal VE ideale to keep a PaCO2 of 37.5 mmHg. Ventilatory Ratio values close to 1 indicate the absence or little relevance of dead space: “ideal” VE is enough to keep normal PaCO2 values, as in physiology.
When Mario has ARDS, Ventilatory ratio becomes:
Ventilatory Ratio = 12 L/min / 7 L/min ∙ 70 mmHg/37.5 mmHg = 3.2.
In other words, in this condition Mario Rossi needs more than three times the ideal VE to maintain a normal PaCO2, a sign of a severe increase in dead space.
A Ventilatory Ratio higher than 2 is associated with an increased risk of death in ARDS patients.
Conclusions
Let’s summarize this post’s key point:
Hypercapnia’s clinical meaning is different whether it is secondary to minute ventilation reduction or to an increase in dead space;
If hypercapnia is secondary to minute volume reduction, it is easily fixed with mechanical ventilation; fixing hypercapnia secondary to a dead space increase might be dangerous for the patient, because it can lead to non-protective ventilation;
The evaluation of dead space is clinically and prognostically useful for ARDS patients;
In clinical practice, corrected minute ventilation and Ventilatory Ratio are appropriate dead space surrogates, which can be obtained in any ICU.
As always, a smile for all of ventilab’s friends.
References:
Dead space physiology
- Robertson HT. Dead space: the physiology of wasted ventilation. Eur Respir J 2015;45:1704–1716.
Association between dead space and mortality in ARDS
- Nuckton TJ, Pittet J-F, Kallet R, Daniel BM, Pittet J-F, Eisner M, Matthay MA. Pulmonary Dead-Space Fraction as a Risk Factor for Death in the Acute Respiratory Distress Syndrome. N Engl J Med 2002;346:1281–1286.
- Cepkova M, Kapur V, Ren X, Quinn T, Zhuo H, Foster E, Liu KD, Matthay MA. Pulmonary Dead Space Fraction and Pulmonary Artery Systolic Pressure as Early Predictors of Clinical Outcome in Acute Lung Injury. Chest 2007;132:836–842.
- Kallet RH, Zhuo H, Liu KD, Calfee CS, Matthay MA, on behalf of the National Heart Lung and Blood Institute ARDS Network Investigators. The Association Between Physiologic Dead-Space Fraction and Mortality in Subjects With ARDS Enrolled in a Prospective Multi-Center Clinical Trial. Respiratory Care 2014;59:1611–1618.
Association between VEcorr/Ventilatory ratio and mortality in ARDS
- Sinha P, Singh S, Hardman JG, Bersten AD, Soni N. Evaluation of the physiological properties of ventilatory ratio in a computational cardiopulmonary model and its clinical application in an acute respiratory distress syndrome population. Br J Anaesth 2014;112:96–101.
- Sinha P, Calfee CS, Beitler JR, Soni N, Ho K, Matthay MA, Kallet RH. Physiologic Analysis and Clinical Performance of the Ventilatory Ratio in Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med 2019;199:333–341.
- Fusina F, Albani F, Bertelli M, Cavallo E, Crisci S, Caserta R, Nguyen M, Grazioli M, Schivalocchi V, Rosano A, Natalini G. Corrected Minute Ventilation Is Associated With Mortality in ARDS Caused by COVID-19. Respir Care 2021;66:619–625.
Dead space in COVID-19 ARDS and ARDS due to other diseases
- Bertelli M, Fusina F, Prezioso C, Cavallo E, Nencini N, Crisci S, Tansini F, Mazzuca Mari L, Hoxha L, Lombardi F, Natalini G. COVID-19 ARDS is characterized by increased dead space ventilation compared with ARDS from other diseases. A cohort study. Respir Care. 2021 Sep;66(9):1406-1415. doi: 10.4187/respcare.08786.