Original post written on 28th May 2022 by Giuseppe Natalini

Some time ago we had Sonia, a young woman who had a car accident, among our patients.
As soon as she arrived to the hospital, Sonia underwent a CT scan which documented a liver laceration with hemoperitoneum, multiple rib fractures with a left pneumothorax and multiple hip bone fractures. In addition to these injuries, Sonia suffered bilateral femoral fractures and a broken forearm.
Immediately after the CT scan, Sonia was taken to the operating room for a laparotomy which had become urgent since, in the meantime, she manifested signs of hemorrhagic shock.
Now Sonia had to start positive pressure mechanical ventilation in presence of a left anterior pneumothorax which extended from the apex to the base of the lung, with a thickness of up to 3 cm (Figure 1).

There’s the widespread opinion that the beginning of positive pressure ventilation can aggravate a pre-existing pneumothorax and that therefore, in these conditions, a chest drain should be put in place before the pneumothorax evolves into a tension pneumothorax (which is a possible event in presence of a one-way valve mechanism).
The belief that mechanical ventilation can be, by itself, more dangerous than spontaneous breathing for the development or worsening of a pneumothorax is, in my opinion, a prejudice without any physiological basis and is not in agreement with data from medical literature. Let’s try to delve into the topic.
Spontaneous breathing, mechanical ventilation and transpulmonary pressure.
The main difference between spontaneous breathing and positive pressure mechanical ventilation is the pressure in the lungs during inspiration: during mechanical ventilation the pressure inside the lungs is higher than the one detected during spontaneous breathing.
Let’s hypothesize that a patient is ventilated without PEEP, with a tidal volume (VT) of 0.5 L and that his respiratory system’s elastance (Ers) is 24 cmH2O/L (which corresponds to a compliance of 42 mL/cmH2O). In Figure 2 we outline the intrapulmonary pressures at the end of expiration and at the end of inspiration in this subject, wheter he is breathing spontaneously or wheter he is mechanically ventilated:

In case of spontaneous breathing, intrapulmonary pressure at the end of inspiration is 0 cmH2O: the distension of the chest wall by the respiratory muscles brings the pressure in the lungs, after having introduced the whole tidal volume, at the same level as atmospheric pressure. If the same tidal volume is brought in the lungs by mechanical ventilation, the pressure in the lungs at the end of inspiration is 12 cmH2O. This number can be obtained with the equation of motion of the respiratory system, which lets us calculate the pressure that must be applied to the respiratory system during ventilation (see also the post written on 24/06/2011, available only in Italian at the moment):
Pappl = Pel + Pres + P0
where Pappl is the pressure that must be applied, Pel is the elastic pressure, Pres is the resistive pressure and P0 is the pressure at the beginning of inspiration.
If PEEP is not used, Pappl = Pel in the instant in which inspiration ends, because in this moment resistive pressure (which is the product of flow and resistance) becomes 0 since flow falls to zero after the whole tidal volume has been inhaled.
The pressure in the lungs at the end of inspiration is therefore the elastic pressure, i.e. the product of elastance and tidal volume:
Pappl = Pel = Ers٠VT = 24 cmH2O/L ٠0.5 L = 12 cmH2O.
If we stop with our analysis at this level, the opinion that mechanical ventilation has a greater risk to aggravate a pneumothorax than spontaneous breathing could be reasonable: the pressure inside the lungs is actually higher during mechanical ventilation and could apparently favor the leakage of air from the lungs.
But this is obviously only an illusion. The pressure that indeed distends the lungs (and which can favor the leakage of air from a pleural lesion) is not the pressure inside the lungs but the difference between the pressure inside and the one outside the lungs, i.e. transpulmonary pressure.
Figure 3 repeats the outline shown in Figure 2, with the addition of the calculated pleural pressure values (that is, the pressure outside the lungs):
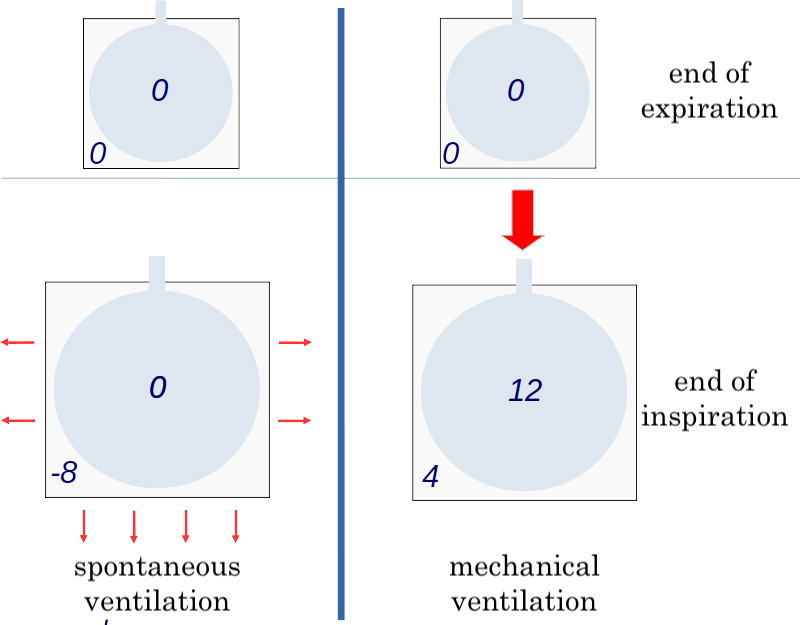
Let’s see how we can calculate pleural pressures in different conditions. We have, for simplicity’s sake, hypothesized that pleural pressure before the beginning of inspiration is 0 cmH2O.
Now let’s calculate pleural pressure at the end of inspiration. To do this, we must know lung elastance (EL) and chest wall elastance (Ecw).
The elastance of the respiratory system is the sum of EL and Ecw:
Ers = EL + Ecw.
Let’s hypothesize that EL is ⅔ of Ers (therefore 16 cmH2O) and that Ecw is ⅓ of Ers (therefore 8 cmH2O), as can be obtained, on average, from physiological studies on the partition of respiratory mechanics between lung and chest wall.
This implicates that ⅔ of the pressure applied to the respiratory system (the one measured in the ventilator) is the pressure that distends the lungs at the end of inspiration (EL٠VT). The "pressure that distends the lungs” is the difference between the pressure inside and outside the lungs, i.e. the pressure in the pleural space.
Similarly, we can calculate that ⅓ of the pressure delivered by the ventilator is necessary to distend the chest wall (Ecw٠VT). The "pressure that distends the chest wall" is the difference between the pressure inside the chest wall (that is, pressure in the pleural space) and the one outside the chest wall, which is atmospheric pressure. Since atmospheric pressure is 0 cmH2O, the "pressure that distends the chest wall" is equal to pleural pressure.
In our example, the pressure that distends the chest wall (Pcw) at the end of inspiration during mechanical ventilation is therefore:
Pcw = Ecw٠VT= 8 cmH2O/L ٠ 0.5 L = 4 cmH2O
This is also the value of pleural pressure that you find in Figure 3 for mechanical ventilation.
The pressure that distends the lung at the end of inspiration in this simulation is 8 cmH2O and not 12 cmH2O, as appeared by looking at Figure 1, which showed only intrapulmonary pressures. Transpulmonary pressure (PL) at the end of inspiration (8 cmH2O), which we have calculated as the difference between pressure inside and outside the lungs, can also be directly calculated, in analogy with previous elastic pressures, as:
PL = EL٠VT = 16 cmH2O/L ٠ 0.5 L = 8 cmH2O.
This formula makes it absolutely clear that transpulmonary pressure at the end of inspiration depends only on tidal volume and lung elastance.
Since these rules are valid for both mechanical ventilation and spontaneous breathing, the pressure that distends the lungs at the end of inspiration will be the same in both conditions if lung elastance and tidal volume are the same.
The only difference between mechanical ventilation and spontaneous breathing is the pump which generates tidal volume: in mechanical ventilation pressure in the lungs is increased by an external machine, during spontaneous breathing pressure outside the lungs is decreased by the respiratory muscles. In this last instance, in order to have a transpulmonary pressure of 8 cmH2O at the end of inspiration, we must have a pleural pressure of - 8 cmH2O. Pleural pressure in the active patient can be calculated from the equation of motion (and in our example it would actually be - 8 cmH2O), but I am going to spare you the calculations. If someone is interested, we can talk about it in the comments section below the post (or in another post).
This is why it is an illusion to think that spontaneous breathing is more protective than mechanical ventilation for the evolution of a pneumothorax. Rather, paradoxically, mechanical ventilation might be preferable in case a spontaneously breathing patient generates a high tidal volume: indeed, with controlled ventilation we can decide to reduce tidal volume and, consequently, transpulmonary pressure.
What happens when we apply PEEP.
Let’s hypothesize that we are applying a PEEP of 12 cmH2O to our hypothetical patient, both during spontaneous breathing and during mechanical ventilation. The situation can be summarized in Figure 4:
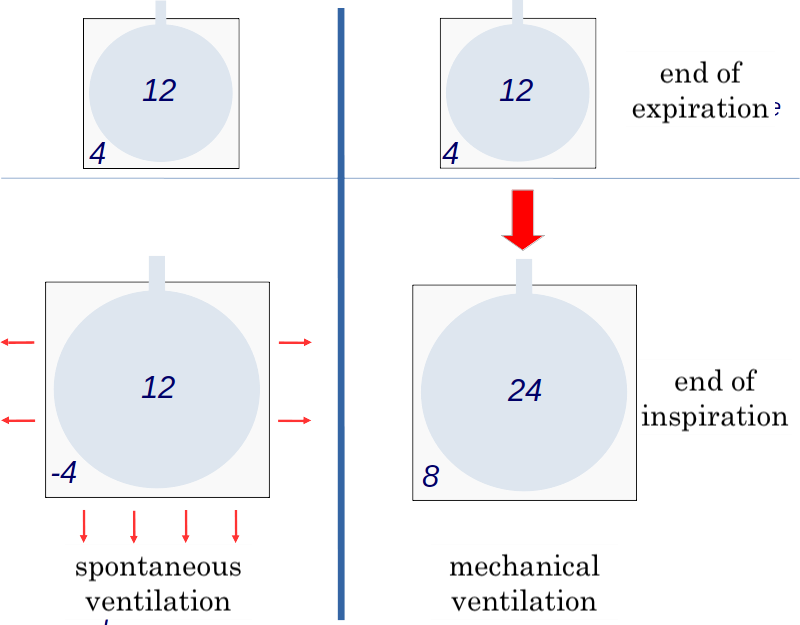
The increase in pleural pressure as a consequence of the increase in airway pressure occurs with the same basis for both the delivery of the tidal volume and the application of PEEP.
Since in our example with assumed that Ecw/Ers = ⅓, the increase in pleural pressure at the end of expiration after the application of PEEP is ⅓ of the applied PEEP. This leads to a transpulmonary pressure, at the end of expiration, of 8 cmH2O in both spontaneous breathing and mechanical ventilation: at the end of expiration there is already a high transpulmonary pressure that favors the emission of air from the lungs.
Repeating the calculations we have already seen for inspiration, we reach a transpulmonary pressure of 16 cmH2O at the end of inspiration, independently for the ventilation modality.
This means that the application of PEEP can effectively contribute to increasing the pneumothorax, but this happens in the same way for spontaneous breathing (for example with CPAP during non invasive ventilation) and for mechanical ventilation.
Pneumothorax and mechanical ventilation: what does medical literature say?
In light of what we have said before, it is not surprising that the frequency of spontaneous pneumothorax and its recurrences (conditions in which no positive pressure ventilation is implied) is especially high for tall and skinny subjects (1,2). During spontaneous breathing, a tall and skinny subject will have the same intra lung pressure as a short and overweight subject, but will reasonably have a lower pleural pressure. The fact that this physical constitution favors spontaneous pneumothorax can be seen as a confirmation that it's not the pressure inside the lungs, but the difference between the pressure inside the lungs and the pleural pressure which favors the development of pneumothorax.
There are several studies on the effects of mechanical ventilation in patients with occult pneumothorax, that is, those forms of anterior pneumothorax which are clearly visible on CT scan but not evident on chest X-rays (as was the case for Sonia).
Medical literature confirms, with both observational studies and randomized and controlled trials, that the clinical evolution of occult pneumothorax is independent of the presence of spontaneous breathing or positive pressure ventilation, and that the frequency of respiratory distress is similar in patients who have a chest drain put in as soon as the occult pneumothorax is diagnosed and in those in whom pleural drainage is reserved for the onset of signs of tension pneumothorax, more frequent in patients receiving long-lasting mechanical ventilation (for more than 5-7 days) (3-7).
What happened to Sonia.
Sonia underwent mechanical ventilation with protective ventilation, without placing a chest drain.
Sonia’s clinical history was very complex, but after about a month in the intensive care unit all issues were satisfactorily resolved and she is now home.
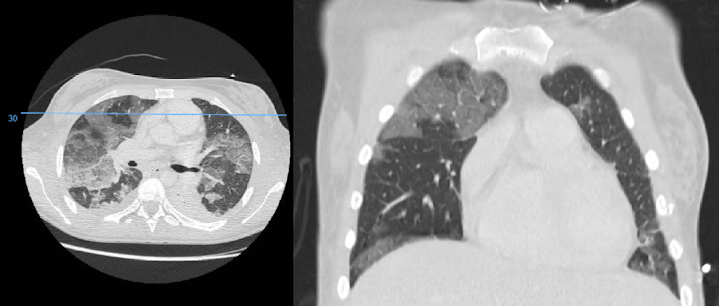
During her stay she had various complications, both pulmonary and extrapulmonary, but the pneumothorax never became a tension pneumothorax and it reabsorbed completely without any medical intervention. In Figure 5 you can see her chest CT scan (with scans similar to the ones seen in Figure 1) after about ten days on mechanical ventilation: you can see an ARDS, but there is no air left outside the lungs.
Conclusions
We can summarize the main messages of this post below:
1) In case of occult and/or clinically not significant pneumothorax, positive pressure mechanical ventilation can be safely started without the placement of a preventive chest tube; clearly, pleural drainage becomes a necessity (sometimes an urgent one) when signs of a tension pneumothorax develop (especially in case of severe hypoxemia and hypotension);
2) If a patient with pneumothorax undergoes mechanical ventilation, tidal volume reduction and intense inspiratory effort abolition make up a protective strategy which reduces the risk of aggravating the pneumothorax compared to a ventilation with high tidal volume/high inspiratory effort (during both spontaneous breathing and mechanical ventilation);
3) In presence of pneumothorax, PEEP should be kept to the minimum necessary value which is compatible with an appropriate mechanical ventilation. Indeed, PEEP can promote an increase in pneumothorax, regardless of spontaneous breathing or mechanical ventilation.
As always, greetings and a smile for all ventilab’s friends.
References
1.Nakamura, H. et al. Physical constitution and smoking habits of patients with idiopathic spontaneous pneumothorax. Jpn J Med 22, 2–8 (1983).
2.Sadikot, R. T., Greene, T., Meadows, K. & Arnold, A. G. Recurrence of primary spontaneous pneumothorax. Thorax 52, 805–809 (1997).
3.Barrios, C. et al. Successful Management of Occult Pneumothorax without Tube Thoracostomy despite Positive Pressure Ventilation. Am Surg 74, 958–961 (2008).
4.Wilson, H., Ellsmere, J., Tallon, J. & Kirkpatrick, A. Occult pneumothorax in the blunt trauma patient: Tube thoracostomy or observation? Injury 40, 928–931 (2009).
5.Kirkpatrick, A. W. et al. Occult pneumothoraces in critical care: A prospective multicenter randomized controlled trial of pleural drainage for mechanically ventilated trauma patients with occult pneumothoraces. J Traum Acute Care Surg 74, 747–755 (2013).
6.Zhang, M., Teo, L. T., Goh, M. H., Leow, J. & Go, K. T. S. Occult pneumothorax in blunt trauma: is there a need for tube thoracostomy? Eur J Trauma Emerg Surg 42, 785–790 (2016).
7.Clements, T. W. et al. OPTICC: A multicentre trial of Occult Pneumothoraces subjected to mechanical ventilation: The final report. Am J Surg 221, 1252–1258 (2021).
No comments:
Post a Comment